Bells Palsy is a weakness of the muscles on one side of the face, often affecting young adults. The palsy is caused by damage to the facial nerve. The nerve can be affected by a number of things. In particular, there can be viral infection causing inflammation and swelling along the nerve which disrupts the relay of muscle activation messages to the facial muscles. The weakness be partial or total. There is often a fatigue or stress component with the viral onset, and the virus itself causes further fatigue.
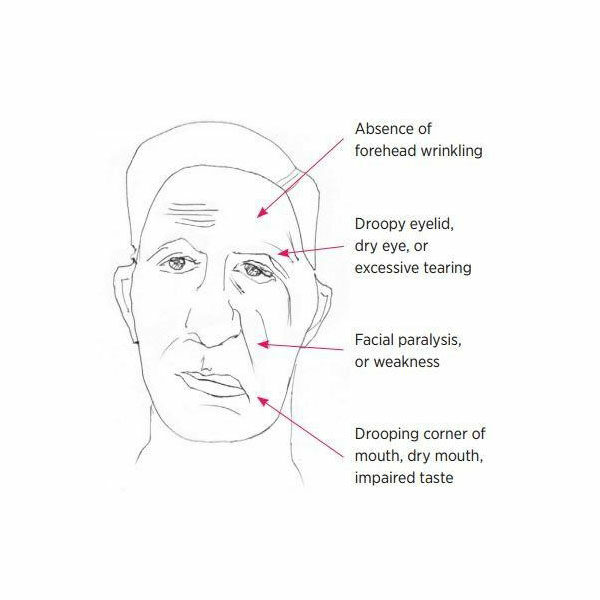
The symptoms of Bell’s palsy are paralysis or weakness on one side of the face, pain around the ear, poor eye closure, and poor capacity to eat and drink. The face feels heavy and can have a numb feeling from the weakness. There can also be a difference in the way food tastes.
Management
The aim of any management is to reduce complications such as damage to the eye and maximise the speed and extent of recovery.
Bell’s palsy usually resolves by itself within a few months and 70% of people will make full recovery without any intervention.
Eye management: Blinking naturally cleans and lubricates the cornea of the eye. If there is incomplete blinking the eye is protected with patching, eye drops and gels.
Medications may be given and have an effect. Prednisolone is a corticosteroid given to reduce the inflammation on the facial nerve. For maximum benefit this needs to start within 72 hours of onset and may continue for up to 10 days. A summary of literature found that prednisolone led to a more complete recovery at 6 months post onset (17% incomplete if had drug and 28% if no drug) and reduction in abnormal muscle activity
Antiviral drug may be given but has so far not shown to be of benefit or add more than what the prednisolone does. (Somasundara and Sullivan, 2017).
Physiotherapy has not been demonstrated to be useful with a lack of controlled studies (Teixeira and Valbuz, 2011). There is low quality evidence that tailored facial exercises can help to improve facial function, mainly for people with moderate paralysis and chronic cases. There is low quality evidence that facial exercise reduces sequelae in acute cases.
At Neurospace we use a range of techniques to help manage the recovery depending on the severity of the weakness and time since onset. The best results are with those we see earliest post onset, but we have seen people 5 years post nerve damage and been able to reduce the severity of the weakness.
Techniques include:
- laser therapy to help manage the inflammation of the nerve,
- muscle stimulator to help the maintain the weak muscles and trigger their activation,
- massage and specific facilitation techniques to maximise muscle activation
- teaching you how to exercise correctly at home and progress the exercises.
Occasionally there are other nerves affected, such as those going to the inner ear and balance system. We help to recognise and diagnosed the symptoms associated vestibular nerve damage and help you to manage this.
Reference
Somasundara D., Sullivan F. Management of Bell’s palsy Aust Prescr 2017;40:94-7 DOI: 10.18773/austprescr.2017.030
Teixeira LJ, Valbuza JS, Prado GF. Physical therapy for Bell’s palsy (idiopathic facial paralysis). Cochrane Database of Systematic Reviews 2011, Issue 12. Art. No.: CD006283. DOI: 10.1002/14651858.CD006283.pub3.